

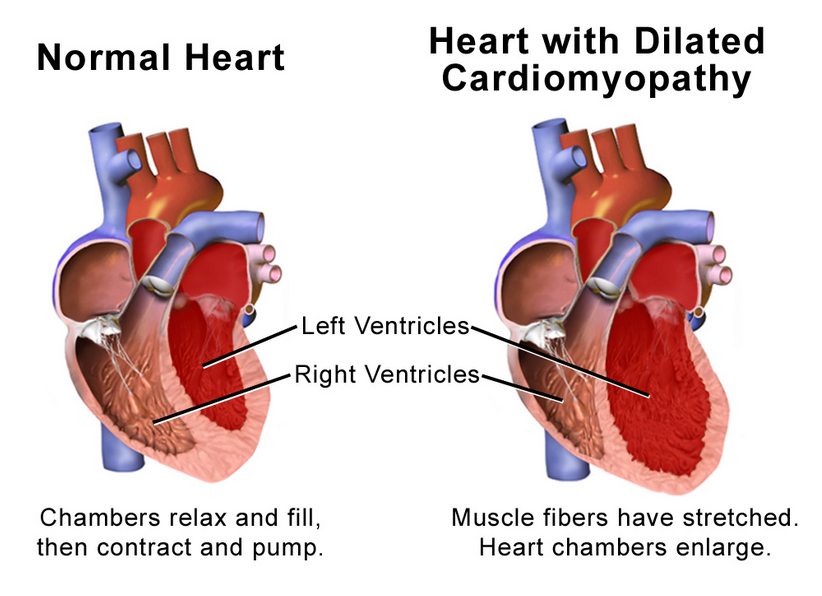
The thickened heart muscle makes it more difficult for the heart to pump out adequate quantities of blood. Source: Blausen.com staff (2014). “Medical gallery of Blausen Medical 2014”. WikiJournal of Medicine 1 (2).
Researchers in the United Kingdom are developed the methodology for a new randomized controlled trial of the efficacy of Coenzyme Q10 adjunctive treatment of heart failure patients.
Two earlier randomized controlled studies have produced results suggesting that daily supplementation with Coenzyme Q10 substantially reduces the morbidity and mortality in patients who are at risk for or have been diagnosed with heart failure.
Q-Symbio Study: Daily supplementation with 300 milligrams of Coenzyme Q10 for two years significantly improved the symptoms, quality of life, and survival of chronic heart failure patients [Mortensen 2014].
KiSel-10 Study: Daily supplementation with a combination of 200 milligrams of Coenzyme Q10 and 200 micrograms of a high-selenium yeast preparation for four years significantly reduced the risk of cardiovascular mortality in senior citizens aged 70 – 88 years [Alehagen 2013]. The protective effect of the intervention persisted through year 12 of follow-up [Alehagen 2018].
Note: A diagnosis of heart failure indicates that the heart is not pumping a sufficient quantity of blood to the other organs and tissues in the body. Heart failure has many different causes and manifestations, the prognosis for heart failure is generally poor, and the heart failure patient’s condition gets progressively worse.
New CoQ10 and heart failure study proposed in the United Kingdom
Now, under the leadership of Professor John Cleland, Glasgow Clinical Trials Unit, Robertson Centre for Biostatistics, Glasgow, Scotland, the steering group for a new Coenzyme Q10 and heart failure study has applied to the British Heart Foundation for funding.
The stated purpose of the new study is to confirm or refute whether Coenzyme Q10 supplementation improves well-being, morbidity, and mortality in a broad range of heart failure patients with or without reduced left ventricular ejection fraction.
Note: Ejection fraction is the cardiologists’ measurement of the percentage of blood leaving a patients’ left ventricle each time the heart muscle contracts. A healthy heart will have an ejection fraction above 50%, meaning that more than half of the blood that fills the left ventricle is pumped out again.
CoQ10 and heart failure study procedures
The steering group for the new UK study of the efficacy of CoQ10 adjuvant treatment of chronic heart failure patients propose the following study procedures:
- screening at 100 UK medical facilities to enroll over 1800 heart failure patients for eligibility to participate in the study
- screening of the heart failure patients for demographics, medical history, medications, quality of life, clinical examinations, hematology and biochemistry tests, NT-proBNP bio-markers for heart failure, walk test, etc.
- drawing and storage of blood for baseline measurements
- random assignment to an active treatment group to take one 100-milligram CoQ10 capsule three times daily or to a placebo group to take a matching placebo capsule three times daily
- dispensing visits for the study participants every three months
- research visits for the study participants at six months
- hazard ratios calculated on the basis of 631 first-events (e.g. hospitalization, heart attack, heart transplantation, cardiac death)
Power calculations for the proposed UK study of CoQ10 and heart failure
With a sample size based on time to first-event, 631 first-events should give the UK researchers 94% power to detect 25% better protection for the Coenzyme Q10 supplementation group as compared to the placebo group.
Similarly, 631 first-events should give the UK researchers 80% to detect 20% protection for the Coenzyme Q10 supplementation group as compared to the placebo group.
In the Q-Symbio study, daily supplementation with 300 milligrams of Coenzyme Q10 was associated with a 43% reduction in the risk of cardiovascular death as compared with placebo supplementation [Mortensen 2014].
Guidelines for the treatment of heart failure patients
From the results of the Q-Symbio study, we know that 300 milligrams of Coenzyme Q10 taken as 100 milligrams three times daily for two years in addition to conventional medication has the following beneficial effects [Mortensen 2014]:
- reduces hospitalization rate
- improves symptoms
- improves survival
If supplementation with 300 milligrams of Coenzyme Q10 daily in the proposed UK study achieves similar results to the Q-Symbio results, then there should be sufficient evidence for the addition of CoQ10 adjunctive treatment of heart failure in the American College of Cardiology/American Heart Association guidelines for the treatment of heart failure [Mortensen 2015].
Coenzyme Q10 adjunctive therapy a positive therapy for heart failure
One important mechanism contributing to the worsening of heart failure may be a dysfunction of cellular bio-energetics caused by the energy starvation of the heart muscle cells [Mortensen 2014].
A second important mechanism contributing to the worsening of heart failure may be insufficient protection against oxidative stress, i.e. the damage caused to heart muscle cells by harmful free radicals [Mortensen 2014].
Coenzyme Q10 molecules are redox molecules. In their oxidized form, Coenzyme Q10 molecules are a key component in the cellular production of ATP energy.
In their reduced form, Coenzyme Q10 molecules provide defense against oxidative stress damage to the heart muscle cells [Mortensen 2014].
Abnormally low plasma CoQ10 concentrations are known to be an independent predictor of mortality in heart failure patients. CoQ10 deficiencies in heart muscle cells are thought to be detrimental to the long-term prognosis of chronic heart failure. Consequently, there is a rationale for adjunctive treatment of heart failure patients with CoQ10 [Molyneux 2008].
CoQ10 supplements safe, affordable, effective but are not all the same
- Coenzyme Q10 supplements are safe and well-tolerated.
- Coenzyme Q10 supplements are affordable.
- Very few Coenzyme Q10 supplements have a documented heart health effect
The formulation of Coenzyme Q10 supplements on the market in the USA, and the resulting absorption and efficacy, varies considerably.
It is undoubtedly wisest to select a Coenzyme Q10 supplement for which there exists scientific documentation of its effect.
Read our key article on CoQ10 as adjuvant therapy for heart failure
Sources
Alehagen, U., Johansson, P., Björnstedt, M., Rosén, A., & Dahlström, U. (2013). Cardiovascular mortality and N-terminal-proBNP reduced after combined selenium and Coenzyme Q10 supplementation: a 5-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. International Journal of Cardiology, 167(5), 1860-1866. doi:10.1016/j.ijcard.2012.04.156
Alehagen, U., Aaseth, J., Alexander, J., & Johansson, P. (2018). Still reduced cardiovascular mortality 12 years after supplementation with selenium and coenzyme Q10 for four years: A validation of previous 10-year follow-up results of a prospective randomized double-blind placebo-controlled trial in elderly. Plos One, 13(4), e0193120. doi:10.1371/journal.pone.0193120
Molyneux SL, Florkowski CM, George PM, et al. (October 2008). “Coenzyme Q10: an independent predictor of mortality in chronic heart failure”. J. Am. Coll. Cardiol. 52 (18): 1435–41. doi:10.1016/j.jacc.2008.07.044.
Mortensen, S. A., Rosenfeldt, F., Kumar, A., Dolliner, P., Filipiak, K. J., Pella, D., & Littarru, G. P. (2014). The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: results from Q-SYMBIO: a randomized double-blind trial. JACC. Heart Failure, 2(6), 641-649.
Mortensen, S. A. (2015). Coenzyme Q10: will this natural substance become a guideline-directed adjunctive therapy in heart failure? Journal of The American College of Cardiology. Heart Failure, 3(3), 270-271.
The information presented in this review article is not intended as medical advice and should not be construed as such.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment