

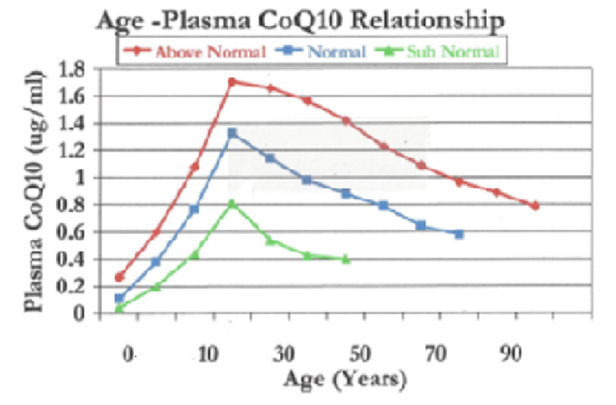
A significant reduction in the rate of CoQ10 biosynthesis has been associated with the aging process and aging-related diseases [Hernandez-Camacho 2018]. It is not possible to make up for this loss of Coenzyme Q10 by eating more selectively. Supplementation with a well-formulated CoQ10 preparation is necessary. (Graph compliments of SIBR Research Institute)
The CoQ10 molecules in the best nutritional supplements are the same molecules as the CoQ10 molecules synthesized inside the mitochondria in human cells.
Absorption and Bio-availability of Coenzyme Q10
Similar to vitamin E, Coenzyme Q10 in food and in nutritional supplements has a low absorption and bio-availability. In the case of Coenzyme Q10, the difficult absorption is attributed to the relatively large size and the lipid soluble nature of the CoQ10 molecules.
Absorption and bio-availability vary greatly from one commercial CoQ10 product to another. Coenzyme Q10 is not the type of product in which the cheaper version is as good as the more expensive version. Developing a 100-milligram CoQ10 supplement that can be absorbed and have a beneficial health effect is a complicated process.
The crystalline CoQ10 raw material has a melting point above 118 degrees Fahrenheit, far higher than the temperatures in the stomach and the small intestines. The manufacturer of a good CoQ10 nutritional supplement must process the CoQ10 raw material in such a way as to ensure that the CoQ10 crystals will dissolve to single molecules at body temperature. The human intestinal absorption cells cannot absorb CoQ10 crystals, only CoQ10 molecules [Judy 2007].
Even when dissolved, CoQ10 molecules are too large to be absorbed directly into the blood. Instead, the CoQ10 molecules that manage to enter the intestinal absorption cells are packed into chylomicrons and released into the lymphatic system. The CoQ10 cells move slowly through the lymph until they reach the thoracic duct near the heart and enter the blood circulation [Judy 2007].
- Absorption of the Coenzyme Q10 in a nutritional supplement will be enhanced by the simultaneous intake of a meal containing some fat.
- Divided doses of Coenzyme Q10, taken with meals, will give a better absorption than single doses. Thus, 2 times 100 milligrams will result in better absorption than 1 time 200 milligrams [Singh 2005].
- Simultaneous intake of Coenzyme Q10 and large dosages of vitamin E (hundreds of milligrams) will attenuate the plasma increase of Coenzyme Q10 and should be avoided [Kaikkonen 2000].
- Supplementation with a well formulated CoQ10 supplement becomes correspondingly more important with increasing age. In the adult years, human cells synthesize less and less Coenzyme Q10 [Kalen 1989].
- Regular long-term use of a CoQ10 nutritional supplement will not affect the ability of human cells to synthesize endogenous Coenzyme Q10 [Folkers 1994].

Dr. William V. Judy, founder and president of SIBR Research Institute, has explained the evidence concerning the absorption, bio-availability, and efficacy of ubiquinone and ubiquinol in his recent book, The Insider’s Guide to Coenzyme Q10. The book can be purchased from amazon.com.
Form and Formulation of CoQ10 Supplements
The Coenzyme Q10 used in nutritional supplements has two forms: the oxidized form called ubiquinone and the reduced form called ubiquinol.
The ubiquinone form has several advantages:
- Ubiquinone has been used far longer than the ubiquinol form.
- Ubiquinone’s absorption, efficacy, and safety are much better documented.
- Ubiquinone is much more stable and much less costly for the supplement manufacturer to process.
- Ubiquinone supplements have been shown to increase significantly the ubiquinol content (i.e. the form needed for antioxidant defense) in plasma and in plasma lipoproteins [Mohr 1992].
- A recent comparison study showed that supplementation with both the ubiquinone form and the ubiquinol form increases the ubiquinol content of the plasma significantly and that there is no significant difference between the plasma ubiquinol increased produced by the one or the other form [Zhang 2018].
- A 2019 comparative bio-availability study showed that the formulation of the CoQ10 supplement is more important than the form (ubiquinone or ubiquinol) of the Coenzyme Q10 used in the supplement [Lopez-Lluch 2019].
Efficacy of CoQ10 Supplements
The best clinical trials of the efficacy of CoQ10 supplements have been done using a pharmaceutical-grade ubiquinone Coenzyme Q10, not a food-grade Coenzyme Q10. The ubiquinone Coenzyme Q10 used in the clinical trials was produced in the same way as medicines are produced [Mortensen 2014; Alehagen 2013]:
- Professor Svend Aage Mortensen’s Q-Symbio study showed that daily supplementation of chronic heart failure patients with 3 times 100 milligrams for two years led to significantly improved symptoms and survival [Mortensen 2014].
- Professor Urban Alehagen’s KiSel-10 study showed that daily supplementation of senior citizens with 2 times 100 milligrams of Coenzyme Q10 in combination with 200 micrograms of a high-selenium yeast preparation for four years led to significantly reduced incidence of death from heart disease, improved symptoms, and improved health-related quality of life [Alehagen 2013].
- Professor Beatrice Golomb’s Gulf War Illness study showed that daily supplementation of patients diagnosed with Gulf War Illness after the first Gulf War with 100 milligrams for three months led to significantly improved physical functions and improved symptoms and quality of life [Golomb 2013].
Safety of CoQ10 Supplements
Properly manufactured Coenzyme Q10 supplements are non-toxic with no observed serious undesirable side effects and no serious interactions with other medications [Hathcock 2006].
The safety of Coenzyme Q10 in healthy adult volunteers has been evaluated in a randomized, double-blind, placebo-controlled study at doses of 300, 600 or 900 mg/day for four weeks. The frequency of adverse events, e.g. common cold symptoms and gastrointestinal effects, was not significantly different between the placebo control and CoQ10 group [Hidaka 2008].
Generally, Coenzyme Q10 was well tolerated at up to 900 milligrams per day, a dosage far higher than the dosage (100 to 300 milligrams daily) needed for therapeutic purposes [Hidaka 2008].
Conclusion: Coenzyme Q10 Supplementation
- Coenzyme Q10 supplements are necessary for cellular energy production, cellular antioxidant protection, and healthy ageing.
- Coenzyme Q10 supplements are safe, effective, and affordable.
- Commercial CoQ10 products are not all the same. Some, by nature of their composition, give a better absorption and bio-availability and, consequently, a better health effect.
Sources
Alehagen, U., Johansson, P., Björnstedt, M., Rosén, A., & Dahlström, U. (2013). Cardiovascular mortality and N-terminal-proBNP reduced after combined selenium and Coenzyme Q10 supplementation: a 5-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. International Journal of Cardiology, 167(5), 1860-1866.
Folkers, K., Moesgaard, S. & Morita, M. (1994). A one-year bioavailability study of Coenzyme Q10 with 3 months withdrawal period. Mol Aspects Med, 15s:s281-s285.
Golomb, B. CoQ10 and Gulf War illness. Neural Computation 2014 Nov; Vol. 26 (11), pp. 2594-651.
Hathcock, J.N. & Shao, A. (2006). Risk assessment for Coenzyme Q10 (Ubiquinone). Regul Toxicol Pharmacol., 45, no. 3, pp. 282-8.
Hernandez-Camacho, J.D., Bernier, M., López-Lluch, G. & Navas, P. (2018). Coenzyme Q10 supplementation in aging and disease. Frontiers in Physiology, 9:44.
Hidaka, T., Fujii, K., Funahashi, I. & Fukotimi, N. & Hosoe, K. (2008). Overview of safety assessment of Coenzyme Q10 (CoQ10). Biofactors, 32(1-4):199-208.
Judy, W. V., Stogsdill, W. W., Judy, D. S., & Judy, J. S. (2007). Coenzyme Q10: Facts or Fabrications? Natural Products Insider. Retrieved from https://www.medicatrix.be/download/ubiquinone_ubiquinol_biodisponibilite.pdf
Kaikkonen, J., Nyyssonen, K., Tomasi, A. & Iannone, A. (2000). Antioxidative efficacy of parallel and combined supplementation with Coenzyme Q10 and d-alpha-tocopherol. Free Radic Res, 33 329-40.
Kalén, A., Appelkvist E.L., Dallner G. (1989). Age-related changes in the lipid compositions of rat and human tissues. Lipids, 24(7):579–584.
López-Lluch, G., Del Pozo-Cruz, J., Sánchez-Cuesta, A., Cortés-Rodríguez, A. B., & Navas, P. (2019). Bioavailability of coenzyme Q10 supplements depends on carrier lipids and solubilization. Nutrition, 57, 133–140.
Mohr, D., Bowry, V. W., & Stocker, R. (1992). Dietary supplementation with Coenzyme Q10 results in increased levels of ubiquinol-10 within circulating lipoproteins and increased resistance of human low-density lipoprotein to the initiation of lipid peroxidation. Biochimica et Biophysica Acta, 1126(3), 247-254.
Mortensen, S. A., Rosenfeldt, F., Kumar, A., Dolliner, P., Filipiak, K. J., Pella, D., & Littarru, G. P. (2014). The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: results from Q-SYMBIO: a randomized double-blind trial. JACC. Heart Failure, 2(6), 641-649.
Mortensen, A. L., Rosenfeldt, F., & Filipiak, K. J. (2019). Effect of Coenzyme Q10 in Europeans with chronic heart failure: A sub-group analysis of the Q-Symbio randomized double-blind study. Cardiology Journal, 26(2): 147-156.
Singh, R. B.,Niaz, M. A., Sindberg, C. D.,Moesgaard, S.,& Littarru, G. P. (2005). Effect of oral coenzyme Q10 dosages on serum Q10 and MDA levels among healthy men. Paper presented at the International Coenzyme Q10AssociationMeeting Abstracts, Los Angeles.
Zhang, Y., Liu, J., Chen, X. & Chen, C-Y. (2018). Ubiquinol is superior to ubiquinone to enhance Coenzyme Q10 status in older men. Food & Function, 9: 5653-5659.
The information presented in this review article is not intended as medical advice and should not be used as such.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment