


Dr. William V. Judy, founder and president of SIBR Research, writes as a guest columnist for Q10facts.com. Dr. Judy has done clinical research in the Coenzyme Q10 adjuvant treatment of patients with heart failure, chronic fatigue syndrome, and prostate cancer. He has supported Prader-Willi children with Coenzyme Q10 therapy. He is the author of the 2018 book Coenzyme Q10: An Insider’s Guide, which is available on amazon.com. ISBN 978-87-7776-186-7.
The question that I get asked about the most is whether there is any benefit from supplementing with Coenzyme Q10 if a person does not have a diagnosed CoQ10 deficiency?
Yes, I think there is a benefit. We should not be waiting until an obvious CoQ10 deficiency manifests itself. Instead, we should be giving people in their 40s and above the following advice:
- Your cells’ bio-synthesis of Coenzyme Q10 will decline with increasing age. Taking various medications, statin medications in particular, will also inhibit your body’s own production of Coenzyme Q10.
- The heart muscle cells need sufficient Coenzyme Q10 to produce enough ATP energy. To prevent the development and worsening of heart disease, you need to take daily CoQ10 supplements to get your plasma CoQ10 levels above 2.0 mcg/mL. If you already have symptoms of heart disease, you probably need to get your plasma CoQ10 levels above 2.5 mcg/mL [Langsjoen 2014].
- Taking 2 or 3 times 100 mg of Coenzyme Q10 daily, together with a meal, for 12 to 24 weeks, should get your plasma CoQ10 levels up to the target level. Firstly, taking more than 100 mg at a time will not bring much extra benefit. Secondly, taking the Coenzyme Q10 together with some fat in a meal will improve the absorption of the Coenzyme Q10.
- You must continue to take CoQ10 supplements even after you reach a plasma concentration of 2.0 mcg/mL. If you stop taking the CoQ10 supplement, your blood levels will decline. Moreover, the Coenzyme Q10 will not go from the blood into the tissue cells unless you have a higher concentration of CoQ10 in the blood.
What is a CoQ10 Deficiency?
In the USA, the normal level of plasma CoQ10 is quoted to be 0.45 to 1.50 mcg/mL. I feel that the 0.45 – 0.60 mcg/mL plasma levels are found in individuals with clinical conditions.
We know that humans’ plasma CoQ10 levels are very variable. For example, the Indian population has generally low plasma levels because of their vegetarian diet. Populations with high protein diets and populations that live is cold climates, on the other hand, tend to have higher plasma CoQ10 levels. But, again, there is considerable individual variability.
What are Symptoms of a Possible CoQ10 Deficiency?
Adequate Coenzyme Q10 in the tissue cells is necessary for cellular energy production. If you are feeling tired even though you have not been exerting yourself physically or mentally, and if sleep is not helping you to feel refreshed and alert, and if you can no longer get as much done during the day as you would like, then you need to consult a physician. A CoQ10 deficiency or insufficiency may be an underlying cause.
Cellular CoQ10 levels appear to be related to the metabolic activity of the cells involved. Heart muscle cells, always working, require constant adequate supplies of Coenzyme Q10. I can’t emphasize this enough.
Plasma and Tissue CoQ10 Levels
Plasma CoQ10 levels are important, but the cellular levels may be even more important. At SIBR Research, for example, we have found low cellular levels of Coenzyme Q10 in patients with chronic fatigue syndrome. Dr. Mortensen and Dr. Folkers found low cellular levels of Coenzyme Q10 in patients with chronic heart failure [Folkers 1985a].
What Comes First, Low CoQ10 Levels or Severe Clinical Conditions?
I believe that CoQ10 deficiencies increase the probability of our developing clinical conditions that are not caused by pathogenic organisms and toxic cellular environments.
It has been shown that CoQ10 supplements can delay the progression of clinical conditions if the supplementation is started early in the onset of the clinical condition [Martelli 2020; Di Lorenzo 2020].
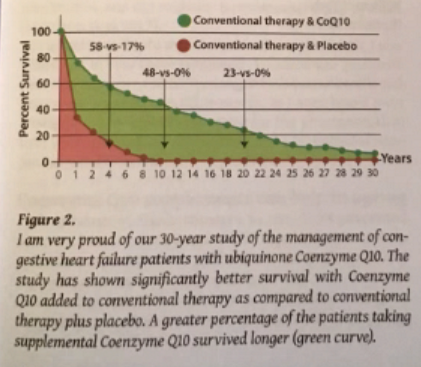
It appears the CoQ10 adjuvant therapy can reverse heart failure and other low-energy clinical conditions [Judy 1986; Mortensen 2014; Mortensen 2019; Alehagen 2013].
The Benefits of CoQ10 Supplementation
As mentioned above, CoQ10 supplementation can improve clinical conditions that are related to a low-energy syndrome; chronic heart disease and chronic fatigue syndrome are prominent among them.
Beyond the obvious clinical conditions, there could be benefits in the maintenance of cellular health as a result of the energy production and antioxidant functions of Coenzyme Q10. Another possibility is the function of Coenzyme Q10 in the immune system [Folkers 1985b].
Moreover, there seems to be some evidence that regular CoQ10 supplementation is associated with reduced levels of systemic inflammation, reduced levels of oxidative stress, and longevity [Alehagen 2015a; Alehagen 2015b; Hernandez-Camacho 2018].
I recall a study in which CoQ10 supplementation increased the antibody response in humans vaccinated against hepatitis B with up to 57% [Barbieri 1999].
We also know that Coenzyme Q10 prevents the mutation of the NQO-1 gene that controls the NQO-1 protein activity that regulates the synthesis of enzymes that drive the CoQ10 redox mechanism [Ross 2017].
Coenzyme Q10 Absorption and Bioavailability
I have no doubt that many of the readers of q10facts.com need a daily CoQ10 supplement.
I want to caution the readers: not all CoQ10 supplements are equally good. Much depends on the formulation of the supplement [Lopez-Lluch 2019]. Thus, documentation of a CoQ10 product’s absorption and bioavailability is important.
Last Word: The Body is a Group of Adaptive Systems
The body is an adaptive group of functional systems. Small function changes are occurring in cells all the time. However, these changes do not cause detectable symptoms. These are what is called silent clinical conditions (hypertension, diabetes, atherosclerosis, neuropathy). Our bodies adapt to the small changes. Thus, we never know what is happening in our cell until the critical level of system failure occurs. It is essential that the energy level and antioxidant functions of all cells are optimal to prevent cell death and to stimulate cell repair. The energizing and antioxidant functions of CoQ10 are essential for maintaining the optimal functional characteristics of the body.
Sources
Alehagen U, Johansson P, Björnstedt M, Rosén A, Dahlström U. Cardiovascular mortality and N-terminal-proBNP reduced after combined selenium and coenzyme Q10 supplementation: a 5-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. Int J Cardiol. 2013 Sep 1;167(5):1860-6.
Alehagen U, Lindahl TL, Aaseth J, Svensson E, Johansson P. Levels of sP-selectin and hs-crp decrease with dietary intervention with selenium and coenzyme Q10 combined: a secondary analysis of a randomized clinical trial. PLoS One. 2015a; 10(9):e0137680.
Alehagen U, Aaseth J, Johansson P. Less increase of copeptin and MR-proADM due to intervention with selenium and coenzyme Q10 combined: Results from a 4-year prospective randomized double-blind placebo-controlled trial among elderly Swedish citizens. Biofactors. 2015b; 41(6):443-52.
Barbieri B, Lund B, Lundström B, Scaglione F. Coenzyme Q10 administration increases antibody titer in hepatitis B vaccinated volunteers–a single blind placebo-controlled and randomized clinical study. Biofactors. 1999;9(2-4):351-7.
Di Lorenzo A, Iannuzzo G, Parlato A, et al. Clinical evidence for Q10 Coenzyme supplementation in heart failure: from energetics to functional improvement. Journal of Clinical Medicine. 2020 Apr;9(5).
Folkers K, Vadhanavikit S, Mortensen SA. Biochemical rationale and myocardial tissue data on the effective therapy of cardiomyopathy with coenzyme Q10. Proc Natl Acad Sci U S A. 1985a;82(3):901-904.
Folkers K, Wolaniuk A. Research on coenzyme Q10 in clinical medicine and in immunomodulation. Drugs Exp Clin Res. 1985b;11(8):539-45.
Hernández-Camacho JD, Bernier M, López-Lluch G, Navas P. Coenzyme Q10 supplementation in aging and disease. Front Physiol. 2018;9:44.
Judy W, Hall J, Toth P. . Double blind-double crossover study of coenzyme Q10 in heart failure. Biomed Clin Aspects Coenzyme Q 1986;5:315–23.
Langsjoen PH, Langsjoen AM. Comparison study of plasma coenzyme Q10 levels in healthy subjects supplemented with ubiquinol versus ubiquinone. Clin Pharmacol Drug Dev. 2014 Jan;3(1):13-7.
Martelli A, Testai L, Colletti A, Cicero AFG. Coenzyme Q10: Clinical applications in cardiovascular diseases. Antioxidants (Basel). 2020;9(4):341.
Mortensen SA, Rosenfeldt F, Kumar A, Dolliner P, Filipiak KJ, Pella D, Alehagen U, Steurer G, Littarru GP; Q-SYMBIO Study Investigators. The effect of coenzyme Q10 on morbidity and mortality in chronic heart failure: results from Q-SYMBIO: a randomized double-blind trial. JACC Heart Fail. 2014 Dec;2(6):641-9.
Mortensen AL, Rosenfeldt F, Filipiak KJ. Effect of coenzyme Q10 in Europeans with chronic heart failure: A sub-group analysis of the Q-SYMBIO randomized double-blind trial. Cardiol J. 2019;26(2):147-156.
Ross D, Siegel D. Functions of NQO1 in Cellular Protection and CoQ10 Metabolism and its Potential Role as a Redox Sensitive Molecular Switch. Front Physiol. 2017;8:595.
The information presented in this article by Dr. Judy is not intended as medical advice and should not be construed as such.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment